It is the amount of fatty tissue that makes some breasts bigger than others. In other words, the milk producing apparatus is about the same in both small and big breasts. Therefore breast size is not linked to the ability to produce breast milk and breastfeed per se. Even flat-chested women, who don't have practically any fat cells in their breasts, can breastfeed. Besides, you really don't know your final breast size until after your first pregnancy, because the milk-producing cells and milk ducts grow and branch out a lot during the third trimester.
However, breast size does affect the breastfeeding relationship in at least two different ways. First of all, many times the babies of large breasted women have some difficulty in latching on in the beginning because they have such a tiny mouth in comparison to the areola they are supposed to take into their mouth and suck on. This problem usually goes away as the baby grows older. A lactation consultant can help with the initial problems; for example, the mother can pump the milk during the early weeks while the baby is learning a proper latch, and the pumped milk can be fed to the baby in a bottle.
Secondarily, the research of Peter Hartmann has shown that the milk storage capacity varies a lot between women. Breast milk is produced continually and it accumulates in the milk ducts between feedings. During feeding, a baby typically empties about 70-80% of the milk in the breast. Hartmann found in his studies that some women had 3 times as big a storage capacity than others - but that all of them produced the same amount of milk over a 24-hour period. In general, bigger breasts of course would have a bigger storage but it was noted that breast size was not always a good predictor of production or storage capacity.
In practical terms it means that women with small storage capacity breasts need to nurse more often, and the babies take in less per feeding. Women whose breasts have a larger storage capacity can 'deliver' more milk in one feeding, and so the baby needs to nurse fewer times per day. This further confirms the need of cue feeding or demand feeding where the baby sets the frequency of breastfeeding - and not the clock or the pediatrician or the grandmother.
During pregnancy, breasts grow a lot in size. This is due to the growth and development of the milk glands. Fat actually goes away from breasts at this time, as the milk glands "fill" the breast. The areola darkens considerably, and breasts already start producing colostrum.
The "peak" size is usually reached when the mature milk comes in about 3-5 days after delivery. At this time most women experience some engorgement, which goes away in a few days. Then, once the breastfeeding relationship is established, breasts will constantly keep changing their size a little bit, as the baby empties the breast, and as milk is constantly being made in the alveoli (milk glands) to fill the breast.
With weaning, when the milk is no longer needed, the milk glands atrophy or shrivel up. The breasts will then shrink in size. If the weaning was abrupt (cold-turkey), this shrinking can be quite marked. However, that is not the end of the story. After weaning, over a period of up to 6 months, the body deposits fat back to the breasts. With gradual weaning, often there isn't any abrupt change in breast size, but the fat-depositing process can take place at the same time with the slow weaning.
With this process of "refilling" with fat, the breasts often end up about the same size as before pregnancy, though they may be hanging down more (saggier). However, some women's breasts do stay smaller than they were before pregnancy.
There is one exception to the rule about breast size/shape and breastfeeding ability, and that is that few women have insufficient glandular tissue (IGT) in their breasts. In other words they simply don't have enough milk producing cells, and these women can then experience milk supply problems.
This condition is also called breast hypoplasia, hypoplastic breasts, or underdeveloped breasts. Often, IGT goes with tubular/tuberous shaped breasts, but not all tubular breasts lack glandular tissue so you cannot judge by appearance alone.

breasts with insufficient glandular tissue
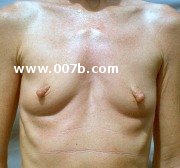
These kind of breasts are underdeveloped (hypoplastic) in terms of the milk glands. They lack normal fullness and may look like 'empty sacks', may be tubular in shape, and may seem bulbous or swollen at the tip. Due to a lack of glandular tissue, hypoplastic breasts are often widely spaced from each other and the breast base is narrow at the chest wall. They often have an elongated or tubular form, and tend to be small. The areola can be enlarged. There may be a significant asymmetry. The breasts don't grow during pregnancy and there is no engorgement when the milk is supposed to come in after giving birth.
These are tubular breasts on an obese woman. They used to be A-cup before she gained a lot of weight.

"I am 28 years old. I have been pregnant once and was unable to breastfeed because I made NO milk. My breasts never changed during pregnancy or engorged after and with the help of a lactation consultant and a hospital grade pump we learned that I made no milk. I am obese and at the time this picture was taken I had lost about 50lbs. I was thin in high school and extremely small chested (maybe an A cup on a good day) and even then they were very saggy. As I gained weight they got bigger though never fuller, just saggier really."
Note, however, that NOT all tubular-shaped breasts are under-developed. Normal breasts CAN also have a tubular shape! So don't go by the shape alone! Insufficient glandular tissue cannot be diagnosed with 100% certainty until a woman has gone through pregnancy, and technically requires a ductogram to confirm. However, if a woman does not have any breast changes during pregnancy and then does not produce enough milk, she may very well suffer from this condition.
These small breasts appear hypoplastic (not having enough glandular tissue) because of the wide gap between them at the chest wall.

However, you can't judge by appearance alone! The proof is in the pudding: the true test of having insufficient glandular tissue is to check if the breasts make enough milk after giving birth.
Scientists don't know for sure the reason(s) for this underdevelopment. One theory is that at least in some women it would be linked to too little progesterone, since progesterone mediates the growth of alveoli (milk-making glands).
In a 2006 study in Mexico, teenage girls who lived in the agricultural valley with heavy pesticide use had poor mammary gland developmend, and 18.5% of them had NO milk glands.
Other issues include PCOS and other insulin metabolism issues, hypothyroidism, and testosterone overload. Fixing the metabolic issues may help, as might pushing lots of stimulation to increase prolactin levels after birth.
There is also one interesting case reproted in the medical literature where a woman with such underdeveloped breasts was able to successfully nurse her second child, after being given natural progesterone during her second pregnancy. Progesterone stimulates the growth of the glandular tissue in breasts during pregnancy.
Also, there exists a very rare genetic condition called "ectodermal dysplasia" which affects the development and function of many parts of the body, including teeth, fingernails, hair, skin, sweat glands, salivary glands and mammary glands. Women with this condition may have insufficient glandular tissue. Read here a comment we received from a breastfeeding mom who has ectodermal dysplacia.
If you happen to have these tubular hypoplastic (under-developed) breasts, talk to a lactation consultant before giving birth. Even better, talk to a doctor before pregnancy about a possible natural progesterone treatment. There are measures you can take to try increase your milk supply and your chances of breastfeeding, such as
Discuss these and other options with the lactation consultant. You may need to supplement with donated breast milk or formula, so it is important to observe the baby's output of wet and dirty diapers and weight gain to make sure the baby is getting enough nutrition. Remember also to be happy for whatever breast milk you produce and not blame yourself - even a little is better than none! And if you don't get any milk at all (which does happen), remember it is not your fault. For this kind of situation we are thankful that the baby formula exists.
Diary of a Lactation Failure
A blog by a lady who suffers from IGT (Insufficient Glandular Tissue). You will find lots of other women's stories with this condition.
LowMilkSupply.org
Information and options to help you reach your breastfeeding goals.
Breastfeeding and underdeveloped (Hypoplastic) breasts from BabyCenter.com
Lactation failure due to insufficient glandular development of the breast Pediatrics. 1985 Nov;76(5):823-8.
Patient with insufficient glandular tissue experiences milk supply increase attributed to progesterone treatment for luteal phase defect.
J Hum Lact. 1999 Dec;15(4):339-43.
In this one case, the woman was able to produce enough milk for her second child when she was treated with natural progesterone during that particular pregnancy. Progesterone stimulates the growth of the glandular tissue in breast (alveoli) during pregnancy.
Altered breast development in young girls from an agricultural environment. Environ Health Perspect. 2006 Mar;114(3):471-5.
"We examined the onset of breast development in a group of
peripubertal girls from the Yaqui Valley of Sonora, Mexico. We observed that
girls from valley towns, areas using modern agricultural practices,
exhibited larger breast fields than those of girls living in the foothills... Further, girls from valley towns displayed a poorly defined relationship between breast size and mammary gland development, whereas girls from the Yaqui foothills, where traditional ranching occurs,
show a robust positive relationship between breast size and mammary size.
... Mammary tissue, determined by palpation, was absent in 18.5% of
the girls living in agricultural areas, although palpable breast adipose
tissue was present."
Altered breast tissue development in young girls linked to pesticides
A news article talking about the lack of mammary glands in the girls exposed to pesticides.